Success is a journey, not the destination. The path continues beyond the peak.
We are all taught how to handle failure. We learn to rise when we fall, to correct mistakes, to be resilient. Entire volumes are devoted to grit, perseverance, and recovery. Yet very few ever teach us how to handle success. And paradoxically, success can be harder to manage than failure.
Success brings light — recognition, joy, new opportunities. But it also casts shadows: complacency, envy, the pressure to repeat achievements, and the danger of losing perspective. Shakespeare captured it perfectly in Henry IV: “Uneasy lies the head that wears the crown.”
To thrive, we must remember that success is a journey, not the destination. Even more, we must accept that success and failure are conjoint twins, two sides of the same coin. One inevitably follows the other, eventually.
Success and Failure: Conjoint Twins
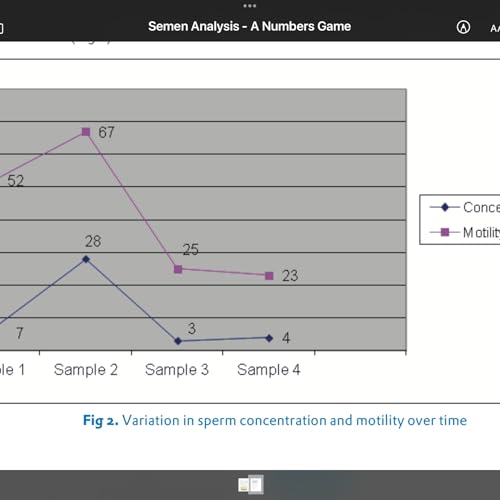
In clinical practice, a new treatment or surgical technique often feels like a triumph. A patient recovers, families rejoice, colleagues congratulate. Yet every doctor knows that early success demands vigilance. Complications may arise. Long-term outcomes must be tracked. In medical research, too, a published paper brings recognition, but it also brings scrutiny. Others will try replication. Critics will probe your methods. A celebrated finding becomes the foundation for the next round of questions, not the end of inquiry.
History echoes this truth. Thomas Edison, often hailed for inventing the light bulb, reframed his countless failed attempts as essential steps: “I have not failed. I have just found 10,000 ways that will not work.”
Lesson: Success and failure are not enemies but twins. Each success carries within it the seeds of future setbacks, and each failure holds the lessons that make future victories possible.
Success Is a Beginning, Not a Destination
One of the greatest conquerors in history, Alexander the Great, wept in his twenties because there were “no more worlds left to conquer.” His victories came so swiftly that success itself became a burden. What he thought was the end turned into a void.
The truth is, every success is a starting point, not a finish line. Winning a gold medal, publishing a landmark paper, or launching a popular product may feel conclusive. But the world keeps moving, and the journey continues.
In modern times, companies like Kodak and Blockbuster remind us of the danger of resting too long on your laurels. They mistook their market dominance for permanence, not adapting when the next chapter arrived. Their success blinded them to change.
Lesson: Treat every victory as a milestone on a continuing road. Celebrate it — but then ask, what comes next?
Humility: The Anchor of Achievement
Success often brings applause, and applause can intoxicate. The antidote is humility.
Humility does not mean pretending achievements do not matter. It means recognizing that they were never achieved alone. Behind every success lies a team..
Consider Marie Curie, the first person ever to win Nobel Prizes in two sciences. Despite her unprecedented recognition, she lived modestly, devoted to her laboratory, and never patented her process for isolating radium, believing that science should serve humanity. Her humility kept her achievements in perspective.
In medicine, too, success is rarely solitary. A successful surgery depends on anesthetists, nurses, and technicians. A research breakthrough relies on data collectors, statisticians, and peer reviewers. Acknowledging this network keeps arrogance at bay and preserves the human ties that make future success possible.
Guard Against Complacency
Failure naturally drives us to work harder. Success, ironically, tempts us to relax. Complacency is the most dangerous shadow cast by achievement.

 3 m
3 m 5 m
5 m 4 m
4 m Oct 9 20255 m
Oct 9 20255 m Oct 5 20255 m
Oct 5 20255 m 7 m
7 m Sep 20 20255 m
Sep 20 20255 m Sep 14 20255 m
Sep 14 20255 m