
GOLD MARK (better than MUDPILES): Anion Gap Metabolic Acidosis Mnemonic
No se pudo agregar al carrito
Add to Cart failed.
Error al Agregar a Lista de Deseos.
Error al eliminar de la lista de deseos.
Error al añadir a tu biblioteca
Error al seguir el podcast
Error al dejar de seguir el podcast

GOLD MARK (better than MUDPILES): Anion Gap Metabolic Acidosis Mnemonic
-
Narrado por:
-
De:
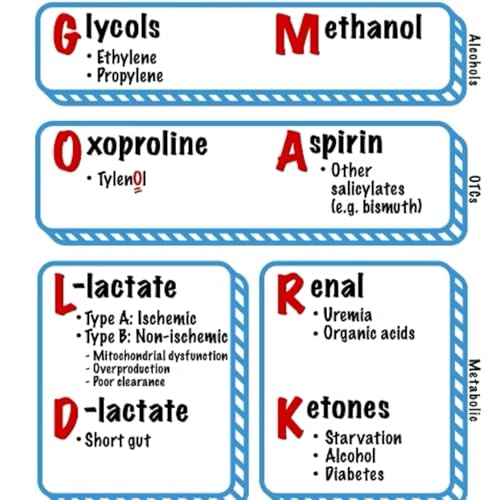
The GOLD MARK causes are divided into three major pathophysiologic groups based on the source of the acid production:
1. Alcohols (Toxic Ingestions) → Emergency Toxins
• Glycols → Ethylene glycol (antifreeze) and propylene glycol
• Methanol → Windshield washer fluid, homemade alcohol substitutes
• Why grouped together?
• Common in suicide attempts, accidental ingestions, or chronic alcoholics.
• Key labs: Serum osmolality, anion gap, osmolar gap.
• Imaging: Calcium oxalate crystals on urine microscopy (ethylene glycol).
• Treatment: Fomepizole or ethanol (blocks alcohol dehydrogenase), hemodialysis in severe cases.
2. OTCs & Medication-Related Causes → Common but Easily Missed
• Oxoproline → Chronic acetaminophen (Tylenol) use, often in malnourished patients
• Aspirin → Salicylates, including bismuth subsalicylate (Pepto-Bismol)
• Why grouped together?
• Often overlooked in chronic users or the elderly.
• Key signs: Tachypnea (respiratory alkalosis), tinnitus (aspirin), altered mental status.
• Key labs: Salicylate level, ABG (mixed acid-base disorder).
• Treatment: Alkalinization (sodium bicarb drip), dialysis for severe cases.
3. Metabolic Causes → Endogenous Acid Production
• L-lactate → Type A (ischemia), Type B (mitochondrial dysfunction)
• D-lactate → Short gut syndrome, bacterial overgrowth
• Renal Failure → Uremia, organic acids
• Ketones → Starvation, alcohol, diabetic ketoacidosis (DKA)
• Why grouped together?
• These involve internal production of acids due to organ dysfunction.
• Key labs:
• Lactate level (for sepsis, ischemia).
• BHB (beta-hydroxybutyrate) for DKA.
• BUN/Cr for renal failure.
• Urinalysis (ketones, glucose, uremia markers).
• Treatment:
• Fluids, treat underlying cause (DKA → insulin drip, renal failure → dialysis).
Clinically Important Considerations for EM Physicians
In the ED, when a patient has metabolic acidosis with an elevated anion gap, think:
1. What is the patient’s history?
• Suicide attempt or confusion? → Alcohols, aspirin
• Chronic Tylenol use or malnourished? → Oxoproline
• Sepsis, shock, ischemia? → L-lactate
• Short gut, diarrhea, recent antibiotics? → D-lactate
• Known diabetes, alcoholism, or fasting? → Ketones
• Chronic kidney disease? → Uremia
2. What tests should I order immediately?
• ABG/VBG → Confirms metabolic acidosis.
• Anion gap calculation → Determines if the acidosis is anion gap or non-anion gap.
• Serum osmolality & osmolar gap → Alcohol toxicity (ethylene glycol, methanol).
• Lactate level → Sepsis, ischemia, mitochondrial dysfunction.
• BHB (Beta-hydroxybutyrate) → DKA vs. alcoholic/starvation ketosis.
• Salicylate level & acetaminophen level → Toxic ingestion screening.
• CMP (BUN/Cr, glucose, liver enzymes, electrolytes) → Renal failure, DKA, liver dysfunction.
Takeaway: What’s an Emergency?
• Dialysis Emergencies → Methanol, ethylene glycol, severe aspirin toxicity, uremia.
• Toxin Emergencies → Alcohols (treat with fomepizole), salicylates (alkalinization & dialysis).
• Septic Shock / Tissue Hypoxia → Elevated L-lactate = immediate resuscitation with fluids & source control!
• DKA → Fluids, insulin drip, and monitor for electrolyte shifts (esp. potassium).